 Acute phase:
Acute phase:
- Time of infection the majority will not have symptoms
- If symptoms develop usually non-specific; fever, enlarged lymph nodes, fatigue
- These non-specific symptoms can last for day to weeks but then resolve
- Chagoma is local inflammation at the site where the parasite entered the skin (can easily be confused with allergy to Kissing bug bite)
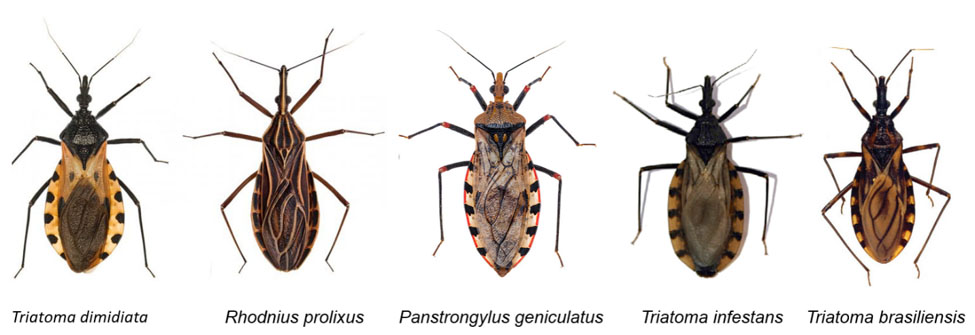
- Remember the Kissing Bug bite DOES NOT transmit the parasite; only the fecal matter of the bug contains the parasite and the kissing bug will need to defecate on you during feeding for transmission to occur if related to a bite.
- Romaña’s sign: swelling around the eye of a person who contracted the parasite through the mucous membranes (not common)
- If a person has an existing weakened the immune system they can develop a serious acute infection such as myocarditis (inflammation of the heart), pericardial effusion (fluid around the heart) and even meningoencephalitis (swelling of the brain and lining).
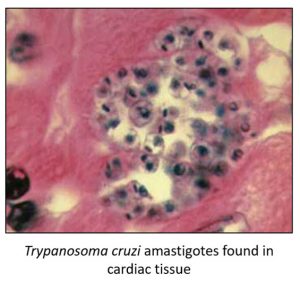
After acute infection we do not know who will clear the infection naturally or who will develop a chronic illness. Unfortunately the testing that is currently available can only determine if you have had exposure to the parasite. These tests primarily look at antibodies (memory proteins produced by certain immune cells in the blood) created against T. cruzi. Sometimes we can detect the parasite through microscopy of blood or tissue samples or other molecular techniques utilized to detect T. cruzi DNA.
This is where things sometimes can get confusing but let’s dive in deeper. If you screen positive and then have positive confirmatory testing done that is specific for exposure to T. cruzi, then you have been exposed and are deemed infected. Since we do not have a test that tells us if you may or may not develop a chronic illness from the parasite, and you do not have any clinical evidence of a disease related to Chagas, you are now classified as being in the “indeterminate phase”.
Indeterminate Phase:
- Do not have any clinical evidence of an illness related to Chagas disease
- Screening and confirmatory testing is positive for exposure to the parasite
- Majority of people will remain without symptoms in their life but sometimes parasite can be detected intermittently in the blood
- If a person develops a condition that weakens the immune system (AIDS, blood cancer, chemotherapy, immune suppressing agents for organ transplantation…) then the parasite can “reactivate” and then cause a serious disease which is sometimes fatal
- People with indeterminate phase of Chagas disease should be monitored with a clinical provider for the development of Chronic Chagas disease.
Chronic Phase:
Chagas heart disease: most common organ involved.
- Will typically lead to abnormal electrical activity (heart block, arrhythmias…)
- Sudden cardiac arrest does occur
- Dilated cardiomyopathy and congestive heart failure (weakened heart)
- Typically take 2-3 decades to clinically recognize heart involvement
Gastrointestinal tract disease: abnormal swallowing and enlargement of esophagus and/or colon
- Progressive trouble swallowing liquids then solids are typically first
- Chronic constipation and abdominal pain; colon will sometimes perforate
- Colon can enlarge and distend the abdomen
Thromboembolic disease: higher rates of pulmonary embolism and stroke have been described among those with chronic Chagas disease.